The following clinically significant adverse reactions are described elsewhere in the monograph: Hypersensitivity and Other Administration Reactions [see Hypersensitivity and Other Administration Reactions under Precautions]; Cardiac Toxicity in Patients with Light Chain (AL) Amyloidosis [see Cardiac Toxicity in Patients with Light Chain (AL) Amyloidosis under Precautions]; Neutropenia [see Neutropenia under Precautions]; Thrombocytopenia [see Thrombocytopenia under Precautions].
Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
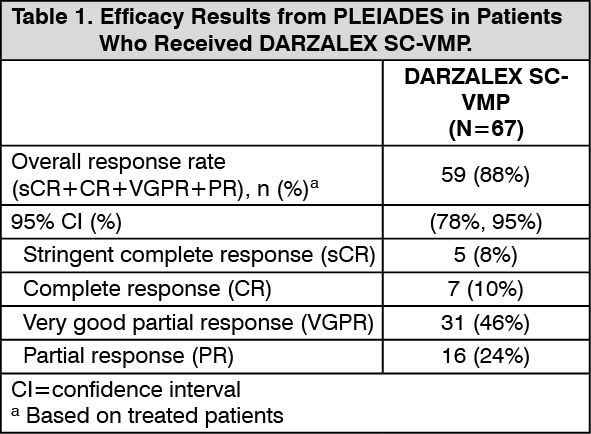
Newly Diagnosed Multiple Myeloma: In Combination with Bortezomib, Melphalan and Prednisone: The safety of DARZALEX SC with bortezomib, melphalan and prednisone was evaluated in a single-arm cohort of PLEIADES [see Pharmacology: Pharmacodynamics: Clinical Studies: Newly Diagnosed Multiple Myeloma under Actions]. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 6, once every 3 weeks from weeks 7 to 54 and once every 4 weeks starting with week 55 until disease progression or unacceptable toxicity (N=67) in combination with bortezomib, melphalan and prednisone. Among these patients, 93% were exposed for 6 months or longer and 19% were exposed for greater than one year.
Serious adverse reactions occurred in 39% of patients who received DARZALEX SC. Serious adverse reactions in >5% of patients included pneumonia and pyrexia. Fatal adverse reactions occurred in 3% of patients.
Permanent discontinuation of DARZALEX SC due to an adverse reaction occurred in 4.5% of patients. The adverse reaction resulting in permanent discontinuation of DARZALEX SC in more than 1 patient was neutropenic sepsis.
Dosage interruptions (defined as dose delays or skipped doses) due to an adverse reaction occurred in 51% of patients who received DARZALEX SC. Adverse reactions requiring dosage interruptions in >5% of patients included thrombocytopenia, neutropenia, anemia, and pneumonia.
The most common adverse reactions (≥20%) were upper respiratory tract infection, constipation, nausea, fatigue, pyrexia, peripheral sensory neuropathy, diarrhea, cough, insomnia, vomiting, and back pain.
Table 13 summarizes the adverse reactions in patients who received DARZALEX SC in PLEIADES. (See Table 13.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Clinically relevant adverse reactions in <10% of patients who received DARZALEX SC with bortezomib, melphalan and prednisone included: General disorders and administration site conditions: infusion reaction, injection site reaction, chills.
Infections: herpes zoster, urinary tract infection, influenza, sepsis.
Musculoskeletal and connective tissue disorders: arthralgia, muscle spasms.
Nervous system disorders: headache, paresthesia.
Metabolism and nutrition disorders: hypocalcemia, hyperglycemia.
Respiratory, thoracic and mediastinal disorders: dyspnea, pulmonary edema.
Cardiac disorders: atrial fibrillation.
Table 14 summarizes the laboratory abnormalities in patients who received DARZALEX SC in PLEIADES. (See Table 14.)
Click on icon to see table/diagram/image
Relapsed/Refractory Multiple Myeloma: In Combination with Lenalidomide and Dexamethasone: The safety of DARZALEX SC with lenalidomide and dexamethasone was evaluated in a single-arm cohort of PLEIADES [see Pharmacology: Pharmacodynamics: Clinical Studies: Relapsed/Refractory Multiple Myeloma under Actions]. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or unacceptable toxicity (N=65) in combination with lenalidomide and dexamethasone. Among these patients, 92% were exposed for 6 months or longer and 20% were exposed for greater than one year.
Serious adverse reactions occurred in 48% of patients who received DARZALEX SC. Serious adverse reactions in >5% of patients included pneumonia, influenza and diarrhea. Fatal adverse reactions occurred in 3.1% of patients.
Permanent discontinuation of DARZALEX SC due to an adverse reaction occurred in 11% of patients who received DARZALEX SC. Adverse reactions resulting in permanent discontinuation of DARZALEX SC in more than 1 patient were pneumonia and anemia.
Dosage interruptions due to an adverse reaction occurred in 63% of patients who received DARZALEX SC. Adverse reactions requiring dosage interruptions in >5% of patients included neutropenia, pneumonia, upper respiratory tract infection, influenza, dyspnea, and blood creatinine increased.
The most common adverse reactions (≥20%) were fatigue, diarrhea, upper respiratory tract infection, muscle spasms, constipation, pyrexia, pneumonia, and dyspnea.
Table 15 summarizes the adverse reactions in patients who received DARZALEX SC in PLEIADES. (See Table 15.)
Click on icon to see table/diagram/image
Clinically relevant adverse reactions in <10% of patients who received DARZALEX SC with lenalidomide and dexamethasone included: Musculoskeletal and connective tissue disorders: arthralgia, musculoskeletal chest pain.
Nervous system disorders: dizziness, headache, paresthesia.
Skin and subcutaneous tissue disorders: rash, pruritus.
Gastrointestinal disorders: abdominal pain.
Infections: influenza, sepsis, herpes zoster.
Metabolism and nutrition disorders: decreased appetite.
Cardiac disorders: atrial fibrillation.
General disorders and administration site conditions: chills, infusion reaction, injection site reaction.
Vascular disorders: hypotension, hypertension.
Table 16 summarizes the laboratory abnormalities in patients who received DARZALEX SC in PLEIADES. (See Table 16.)
Click on icon to see table/diagram/image
In Combination with Pomalidomide and Dexamethasone: The safety of DARZALEX SC with pomalidomide and dexamethasone compared to pomalidomide and dexamethasone (Pd) in patients who had received at least one prior line of therapy with lenalidomide and a proteasome inhibitor (PI) was evaluated in APOLLO [see Pharmacology: Pharmacodynamics: Clinical Studies: Relapsed/Refractory Multiple Myeloma under Actions]. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or unacceptable toxicity in combination with pomalidomide and dexamethasone (n=149) or pomalidomide and dexamethasone (n=150). Among patients receiving DARZALEX SC-Pd, 71% were exposed for 6 months or longer and 50% were exposed for greater than one year.
Serious adverse reactions occurred in 50% of patients who received DARZALEX SC-Pd. The most frequent serious adverse reactions in >5% of patients who received DARZALEX SC-Pd were pneumonia (15%) and lower respiratory tract infection (12%). Fatal adverse reactions occurred in 7% of patients who received DARZALEX SC-Pd.
Permanent treatment discontinuation due to an adverse reaction occurred in 2% of patients who received DARZALEX SC-Pd.
The most common adverse reactions (≥20%) were fatigue, pneumonia, upper respiratory tract infection, and diarrhea.
Table 17 summarizes the adverse reactions in patients who received DARZALEX SC in APOLLO. (See Table 17.)
Click on icon to see table/diagram/image
Clinically relevant adverse reactions in <10% of patients who received DARZALEX SC with pomalidomide and dexamethasone include: Metabolism and nutrition disorders: hypocalcemia, hypokalemia, decreased appetite, dehydration.
Nervous system disorders: peripheral sensory neuropathy, syncope, headache, paresthesia, dizziness.
Musculoskeletal and connective tissue disorders: muscle spasms, musculoskeletal chest pain, arthralgia.
Psychiatric disorders: insomnia.
Gastrointestinal disorders: nausea, abdominal pain, vomiting.
Skin and subcutaneous tissue disorders: rash, pruritus.
Cardiac disorders: atrial fibrillation.
General disorders and administration site conditions: infusion reactions, chills, injection site reaction.
Infections: urinary tract infection, influenza, hepatitis B reactivation, herpes zoster, sepsis.
Vascular disorders: hypertension, hypotension.
Table 18 summarizes the laboratory abnormalities in patients who received DARZALEX SC in APOLLO. (See Table 18.)
Click on icon to see table/diagram/image
In Combination with Carfilzomib and Dexamethasone: The safety of DARZALEX SC with carfilzomib and dexamethasone was evaluated in a single-arm cohort of PLEIADES [see Pharmacology: Pharmacodynamics: Clinical Studies: Relapsed/Refractory Multiple Myeloma under Actions]. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from Weeks 1 to 8, once every 2 weeks from Weeks 9 to 24 and once every 4 weeks starting with Week 25 until disease progression or unacceptable toxicity (N=66) in combination with carfilzomib and dexamethasone. Among these patients, 77% were exposed for 6 months or longer and 27% were exposed for greater than one year.
Serious adverse reactions occurred in 27% of patients who received DARZALEX SC in combination with carfilzomib and dexamethasone. Fatal adverse reactions occurred in 3% of patients who received DARZALEX SC in combination with carfilzomib and dexamethasone.
Permanent discontinuation of DARZALEX SC due to an adverse reaction occurred in 6% of patients who received DARZALEX SC.
Dosage interruptions due to an adverse reaction occurred in 46% of patients who received DARZALEX SC.
The most common adverse reactions (≥20%) were upper respiratory tract infection, fatigue, insomnia, hypertension, diarrhea, cough, dyspnea, headache, pyrexia, nausea and edema peripheral.
Table 19 summarizes the adverse reactions in patients who received DARZALEX SC with carfilzomib and dexamethasone (DARZALEX SC-Kd) in PLEIADES. (See Table 19.)
Click on icon to see table/diagram/image
Clinically relevant adverse reactions in <10% of patients who received DARZALEX SC with carfilzomib and dexamethasone include: Gastrointestinal disorders: abdominal pain, constipation, pancreatitis.
Infection and infestations: pneumonia, influenza, urinary tract infection, herpes zoster, sepsis.
Metabolism and nutrition disorders: hyperglycemia, decreased appetite, hypocalcemia.
Musculoskeletal and connective tissue disorders: muscle spasms, arthralgia.
Nervous system disorders: paresthesia, dizziness, syncope.
General disorders and administration site conditions: injection site reaction, infusion reactions, chills.
Skin and subcutaneous tissue disorders: rash, pruritus.
Cardiac disorders: cardiac failure.
Vascular disorders: hypotension.
Table 20 summarizes the laboratory abnormalities in patients who received DARZALEX SC with carfilzomib and dexamethasone in PLEIADES. (See Table 20.)
Click on icon to see table/diagram/image
Monotherapy: The safety of DARZALEX SC as monotherapy was evaluated in COLUMBA [see Pharmacology: Pharmacodynamics: Clinical Studies: Relapsed/Refractory Multiple Myeloma under Actions]. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously or daratumumab 16 mg/kg administered intravenously; each administered once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or unacceptable toxicity. Among patients receiving DARZALEX SC, 37% were exposed for 6 months or longer and 1% were exposed for greater than one year.
Serious adverse reactions occurred in 26% of patients who received DARZALEX SC. Fatal adverse reactions occurred in 5% of patients. Fatal adverse reactions occurring in more than 1 patient were general physical health deterioration, septic shock, and respiratory failure.
Permanent discontinuation due to an adverse reaction occurred in 10% of patients who received DARZALEX SC. Adverse reactions resulting in permanent discontinuation of DARZALEX SC in more than 2 patients were thrombocytopenia and hypercalcemia.
Dosage interruptions due to an adverse reaction occurred in 26% of patients who received DARZALEX SC. Adverse reactions requiring dosage interruption in >5% of patients included thrombocytopenia.
The most common adverse reaction (≥20%) was upper respiratory tract infection.
Table 21 summarizes the adverse reactions in COLUMBA. (See Table 21.)
Click on icon to see table/diagram/image
Clinically relevant adverse reactions in <10% of patients who received DARZALEX SC included: General disorders and administration site conditions: injection site reaction, peripheral edema.
Musculoskeletal and connective tissue disorders: arthralgia, musculoskeletal chest pain, muscle spasms.
Gastrointestinal disorders: constipation, vomiting, abdominal pain.
Metabolism and nutrition disorders: decreased appetite, hyperglycemia, hypocalcemia, dehydration.
Psychiatric disorders: insomnia.
Vascular disorders: hypertension, hypotension.
Nervous system disorders: dizziness, peripheral sensory neuropathy, paresthesia.
Infections: bronchitis, influenza, urinary tract infection, herpes zoster, sepsis, hepatitis B virus reactivation.
Skin and subcutaneous tissue disorders: pruritus, rash.
Cardiac disorders: atrial fibrillation.
Respiratory, thoracic and mediastinal disorders: pulmonary edema.
Table 22 summarizes the laboratory abnormalities in COLUMBA. (See Table 22.)
Click on icon to see table/diagram/image
Light Chain Amyloidosis: In Combination with Bortezomib, Cyclophosphamide and Dexamethasone: The safety of DARZALEX SC with bortezomib, cyclophosphamide and dexamethasone (DARZALEX SC-VCd) was evaluated in ANDROMEDA [see Pharmacology: Pharmacodynamics: Clinical Studies: Light Chain Amyloidosis under Actions]. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or unacceptable toxicity or a maximum of 2 years. Among patients who received DARZALEX SC-VCd, 74% were exposed for 6 months or longer and 32% were exposed for greater than one year.
Serious adverse reactions occurred in 43% of patients who received DARZALEX SC in combination with VCd. Serious adverse reactions that occurred in at least 5% of patients in the DARZALEX SC-VCd arm were pneumonia (9%), cardiac failure (8%), and sepsis (5%). Fatal adverse reactions occurred in 11% of patients. Fatal adverse reactions that occurred in more than one patient included cardiac arrest (4%), sudden death (3%), cardiac failure (3%), and sepsis (1%).
Permanent discontinuation of DARZALEX SC due to an adverse reaction occurred in 5% of patients. Adverse reactions resulting in permanent discontinuation of DARZALEX SC in more than one patient were pneumonia, sepsis, and cardiac failure.
Dosage interruptions (defined as dose delays or skipped doses) due to an adverse reaction occurred in 36% of patients who received DARZALEX SC. Adverse reactions which required a dosage interruption in ≥3% of patients included upper respiratory tract infection (9%), pneumonia (6%), cardiac failure (4%), fatigue (3%), herpes zoster (3%), dyspnea (3%), and neutropenia (3%).
The most common adverse reactions (≥20%) were upper respiratory tract infection, diarrhea, peripheral edema, constipation, fatigue, peripheral sensory neuropathy, nausea, insomnia, dyspnea, and cough.
Table 23 as follows summarizes the adverse reactions in patients who received DARZALEX SC in ANDROMEDA. (See Table 23.)
Click on icon to see table/diagram/image
Clinically relevant adverse reactions not included in Table 23 and occurred in patients who received DARZALEX SC with bortezomib, cyclophosphamide and dexamethasone included: Skin and subcutaneous tissue disorders: rash, pruritus.
Nervous system disorders: paresthesia.
General disorders and administration site conditions: infusion reaction, chills.
Cardiac disorders: cardiac failure
a, cardiac arrest.
Metabolism and nutrition disorders: hyperglycemia, hypocalcemia, dehydration.
Infections: bronchitis, herpes zoster, sepsis, urinary tract infection, influenza.
Vascular disorders: hypertension.
Musculoskeletal and connective tissue disorders: musculoskeletal chest pain.
Gastrointestinal disorders: pancreatitis.
Respiratory, thoracic and mediastinal disorders: pulmonary edema.
a Cardiac failure includes cardiac dysfunction, cardiac failure, cardiac failure congestive, cardiovascular insufficiency, diastolic dysfunction, pulmonary edema, and left ventricular dysfunction occurred in 11% of patients.
Table 24 summarizes the laboratory abnormalities in patients who received DARZALEX SC in ANDROMEDA. (See Table 24.)
Click on icon to see table/diagram/image
Cardiac Adverse Reactions in Light Chain (AL) Amyloidosis: Among patients who received DARZALEX SC in combination with VCd, 72% of patients had baseline cardiac involvement with Mayo Cardiac Stage I (3%), Stage II (46%) and Stage III (51%). Serious cardiac disorders occurred in 16% of patients (8% of patients with Mayo Cardiac Stage I and II and 28% of patients with Stage III). Serious cardiac disorders in >2% of patients included cardiac failure (8%), cardiac arrest (4%) and arrhythmia (4%). Fatal cardiac disorders occurred in 10% of patients (5% of patients with Mayo Cardiac Stage I and II and 19% of patients with Stage III) who received DARZALEX SC in combination with VCd. Fatal cardiac disorders that occurred in more than one patient in the DARZALEX SC-VCd arm included cardiac arrest (4%), sudden death (3%), and cardiac failure (3%).
Immunogenicity: As with all therapeutic proteins, there is the potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies in the studies described as follows with the incidence of antibodies in other studies or to other daratumumab products or other hyaluronidase products may be misleading.
In patients with multiple myeloma and light chain (AL) amyloidosis who received DARZALEX SC as monotherapy or as part of a combination therapy, less than 1% of 819 patients developed treatment-emergent anti-daratumumab antibodies.
In patients with multiple myeloma and light chain (AL) amyloidosis who received DARZALEX SC as monotherapy or as part of a combination therapy, 7% of 812 patients developed treatment-emergent anti-rHuPH20 antibodies. The anti-rHuPH20 antibodies did not appear to affect daratumumab exposure. None of the patients who tested positive for anti-rHuPH20 antibodies tested positive for neutralizing antibodies.
Postmarketing Experience: The following adverse reactions have been identified with post-approval use of daratumumab. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Immune System: Anaphylactic reaction, Systemic administration reactions (including death).
Gastrointestinal: Pancreatitis.
Infections: Cytomegalovirus, Listeriosis.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image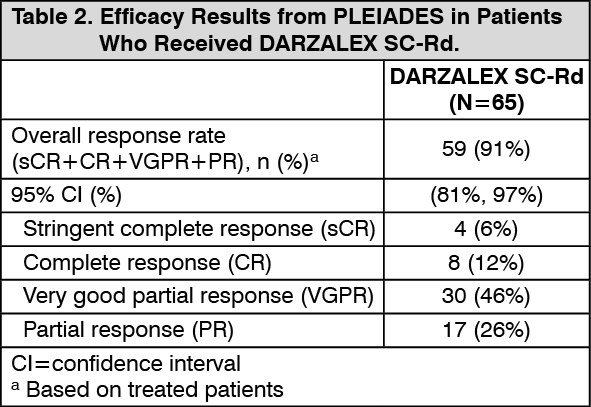 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image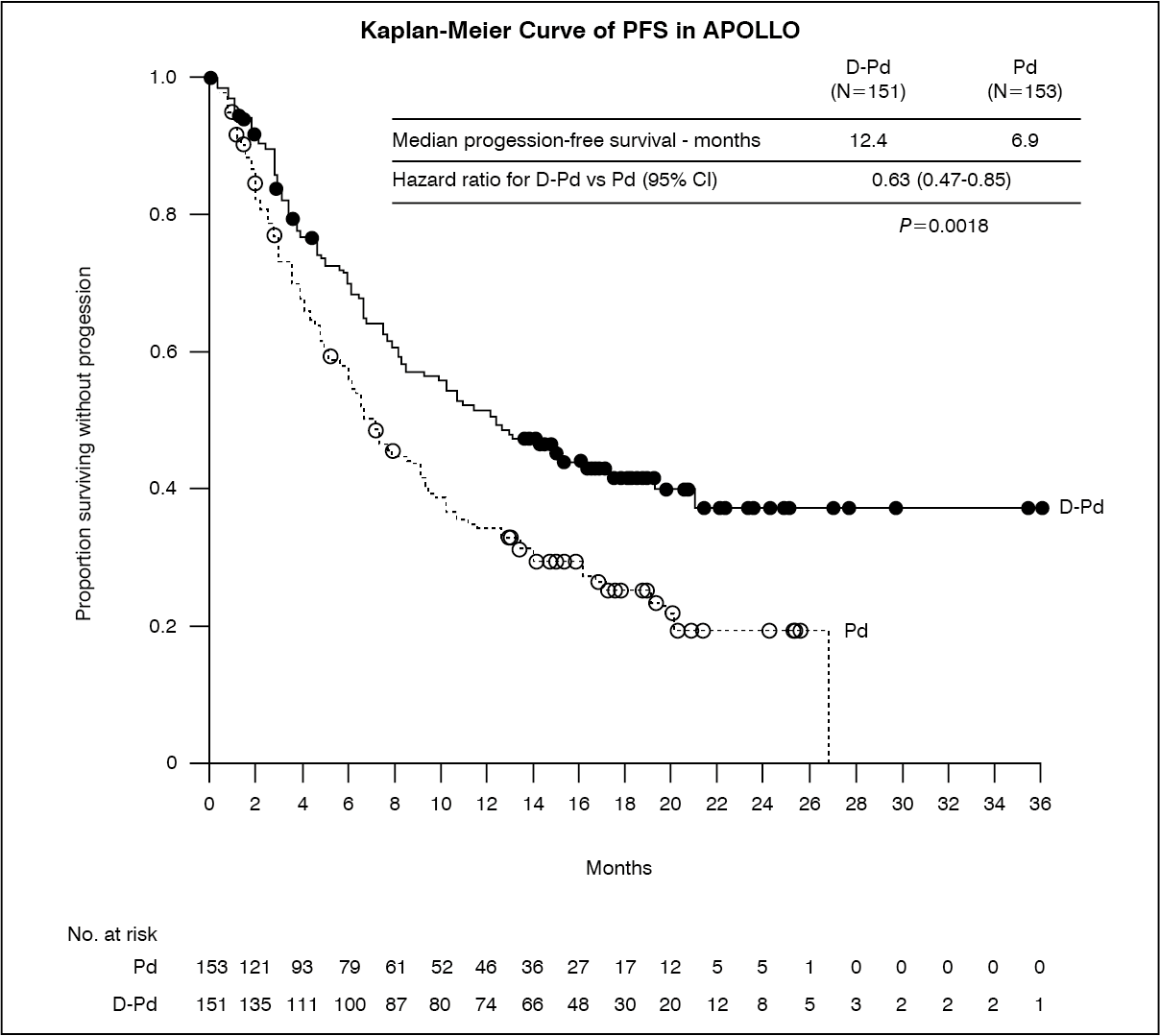 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image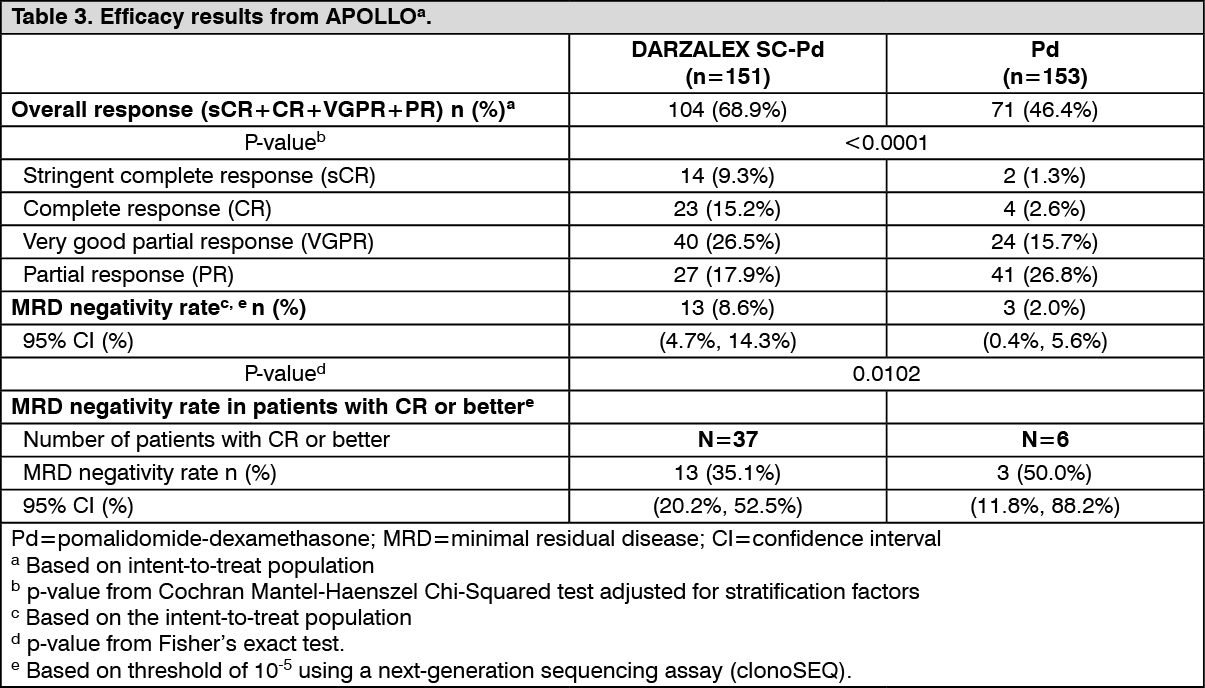 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image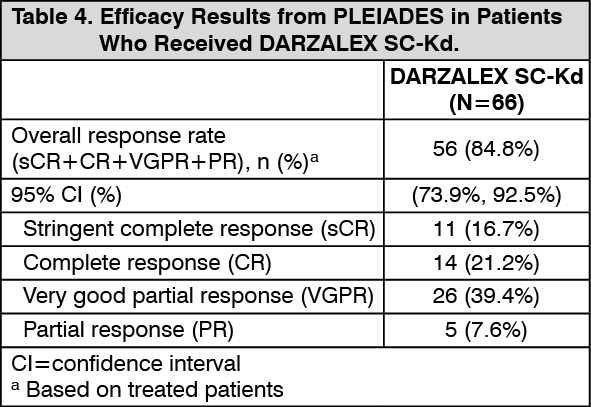 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image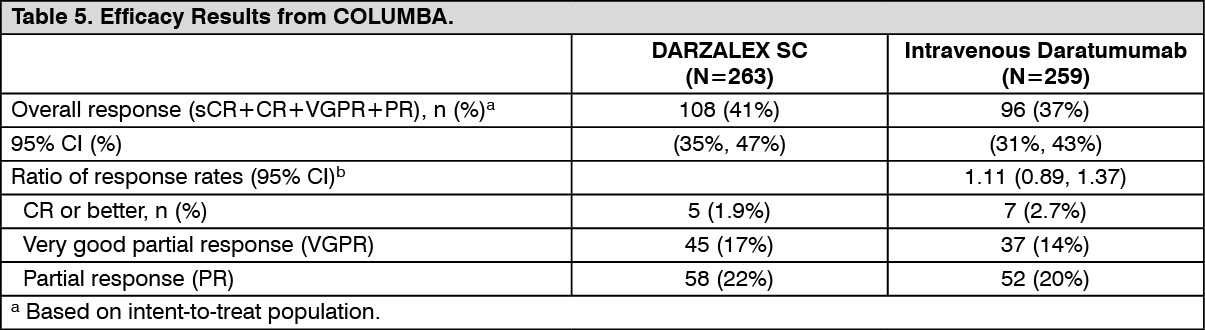 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image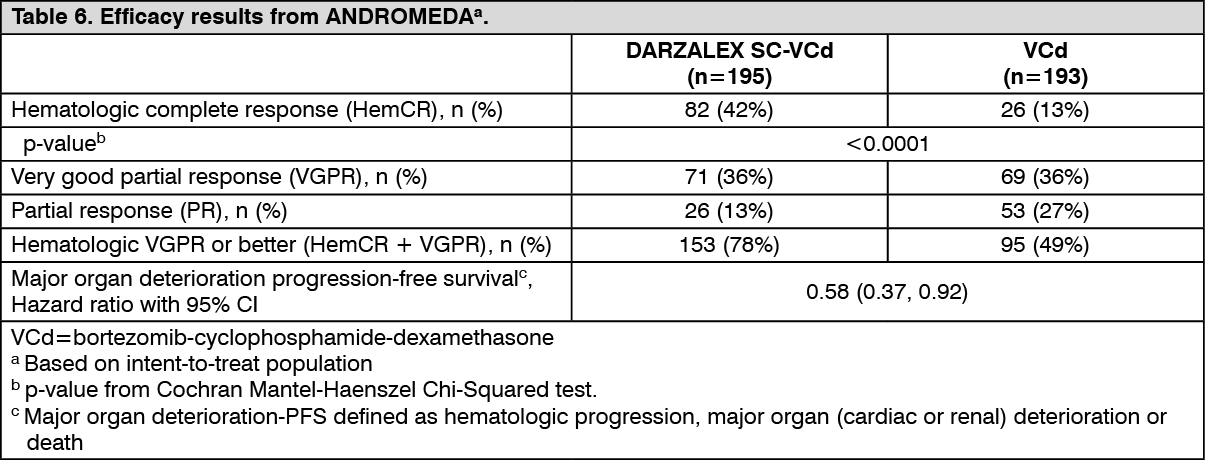 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image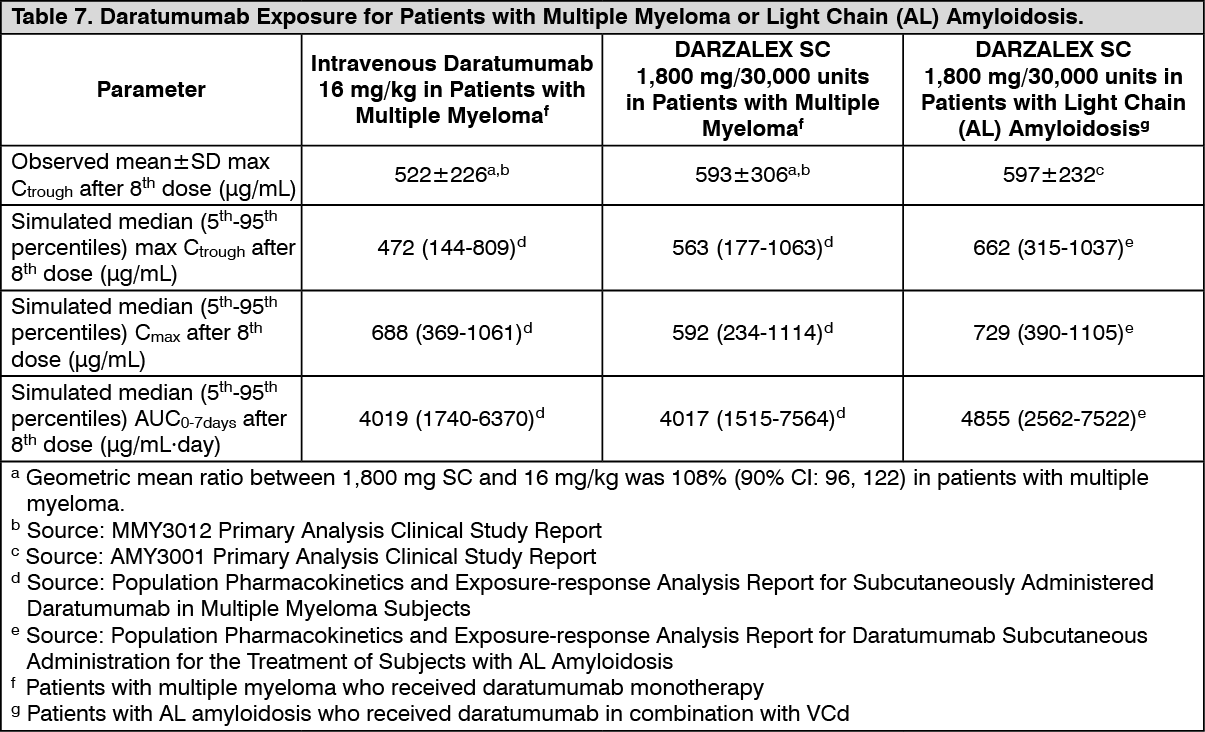 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image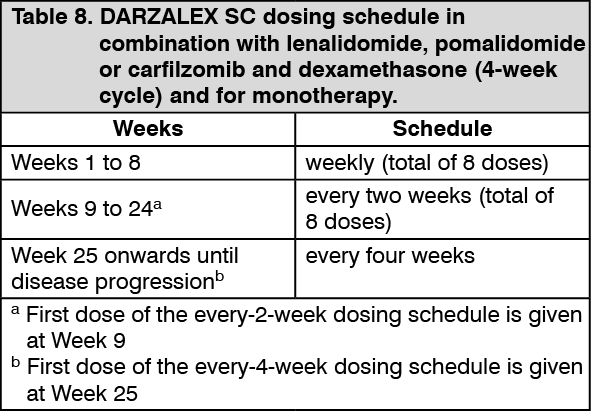 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image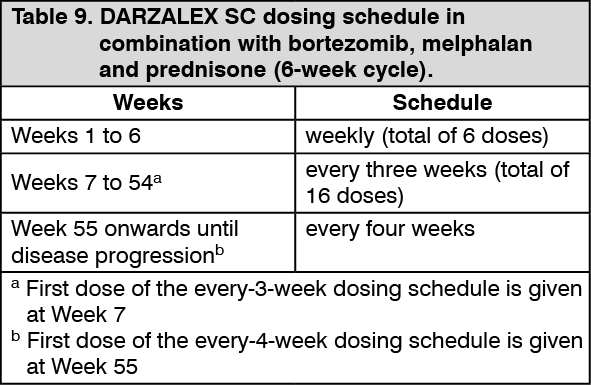 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image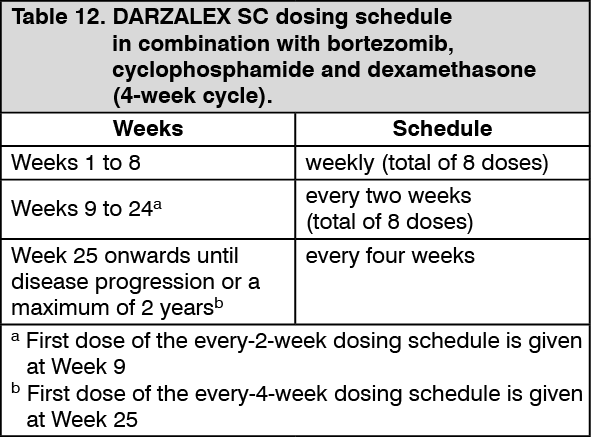 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image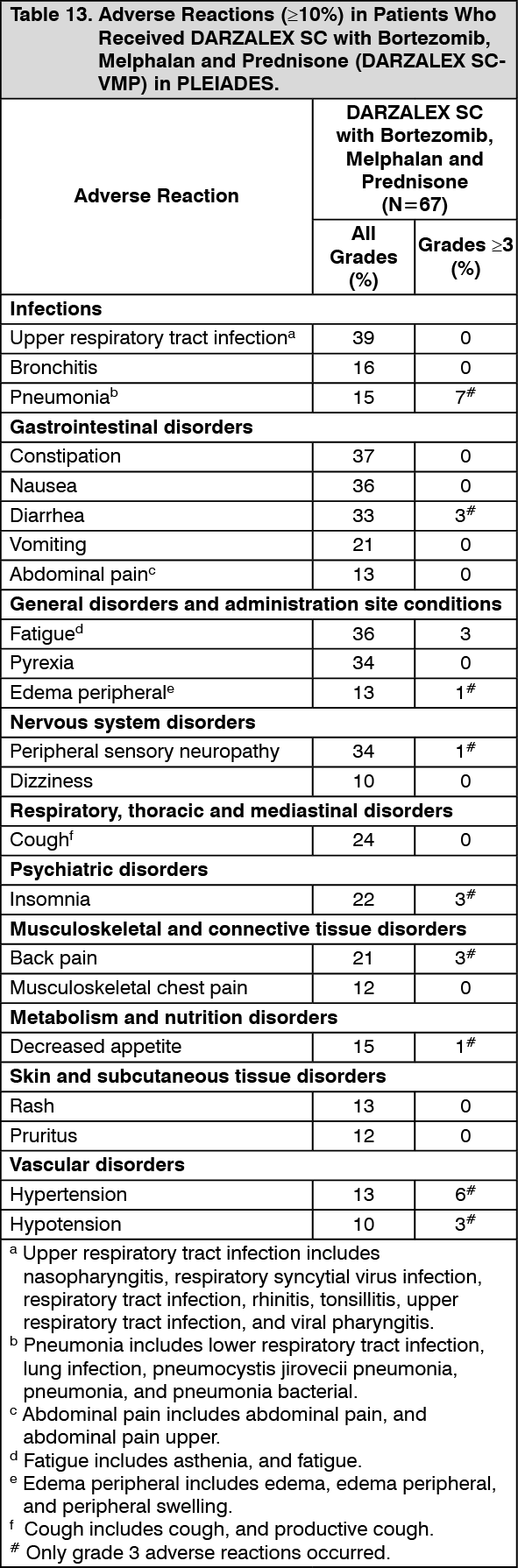 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image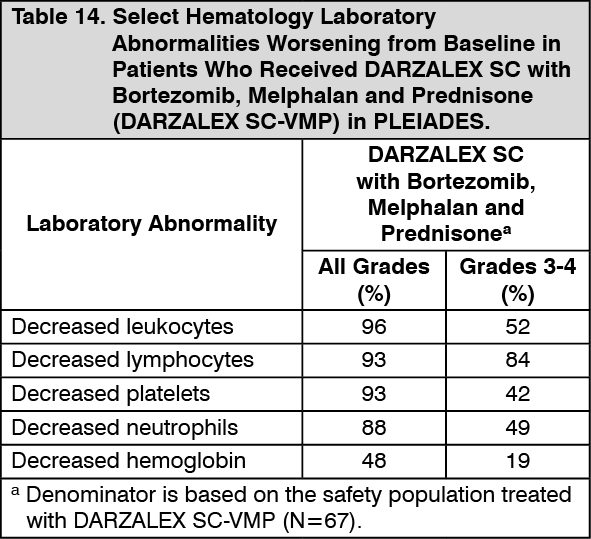 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image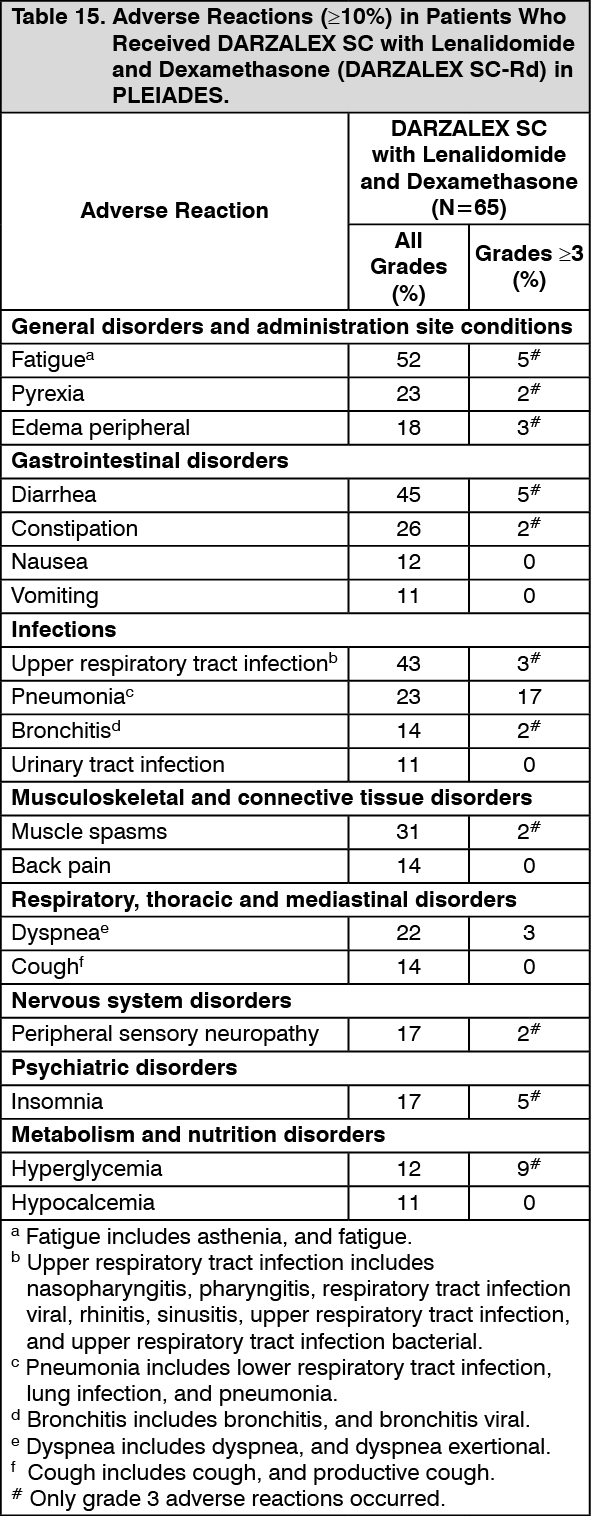 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image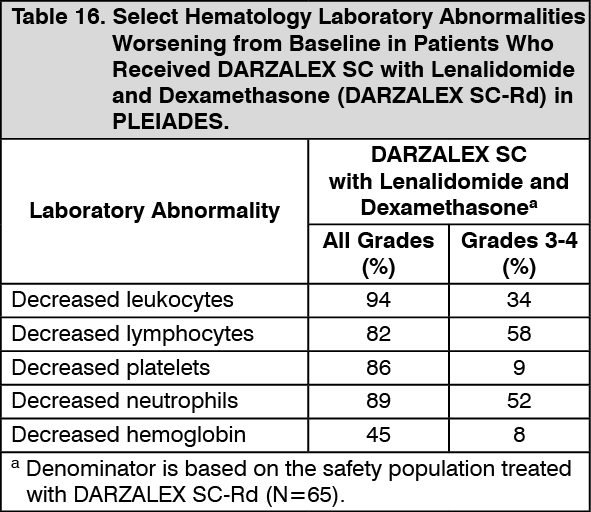 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image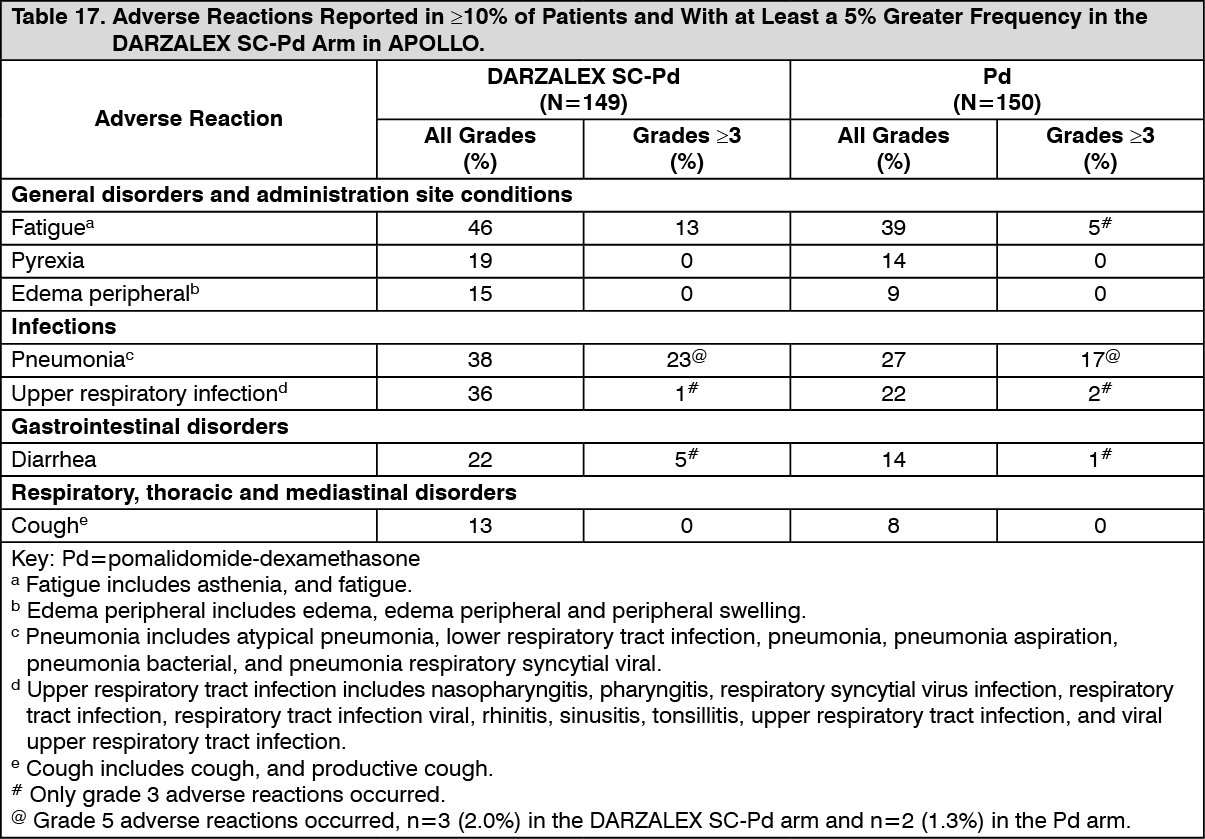 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image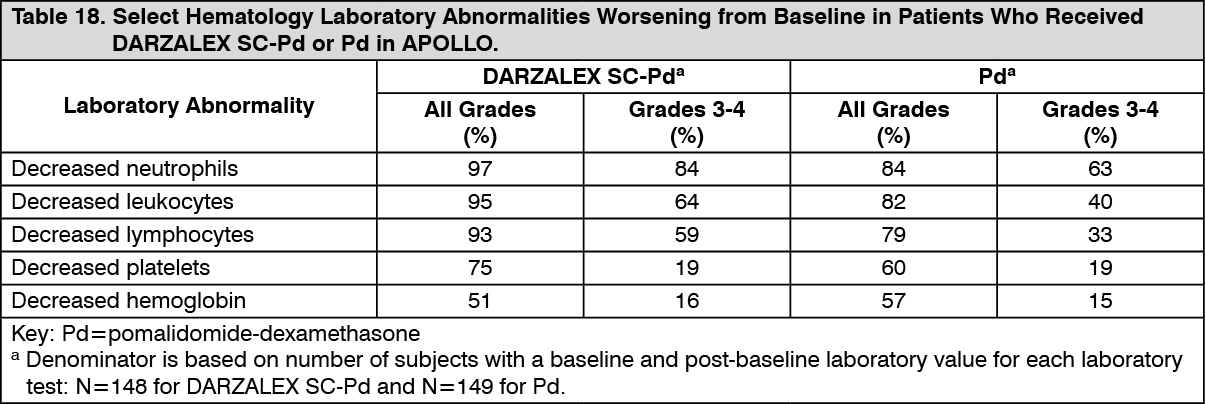 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image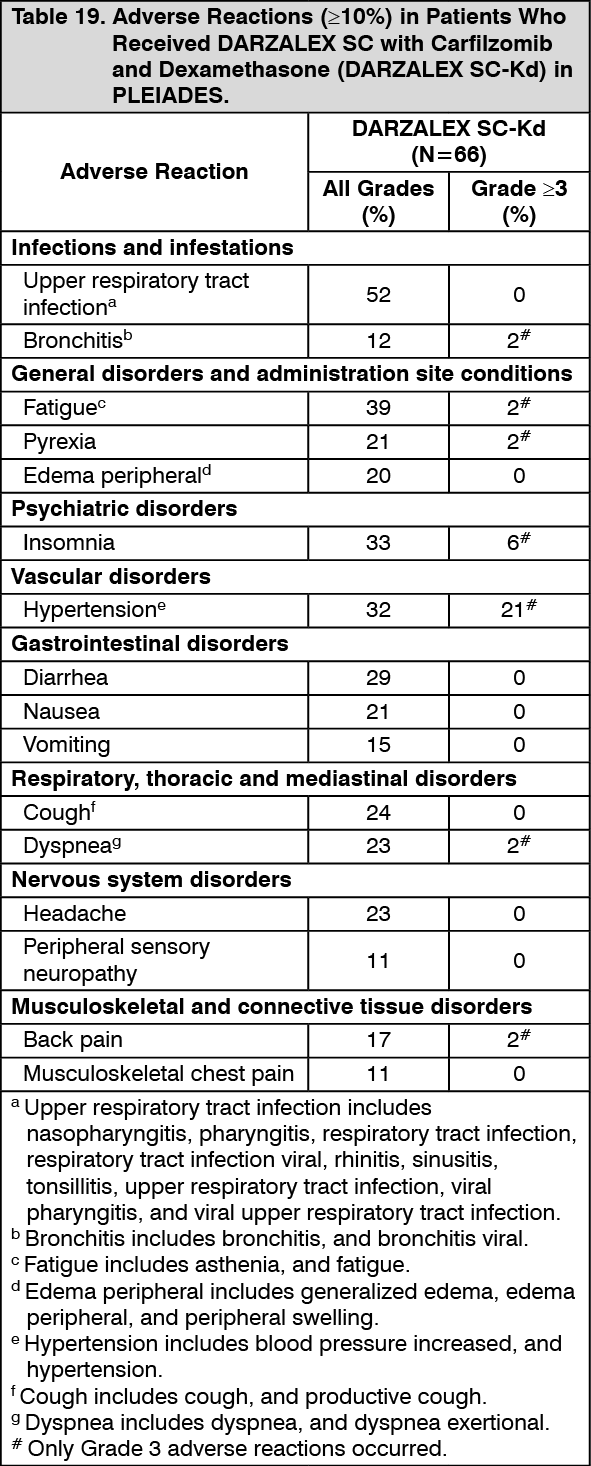 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image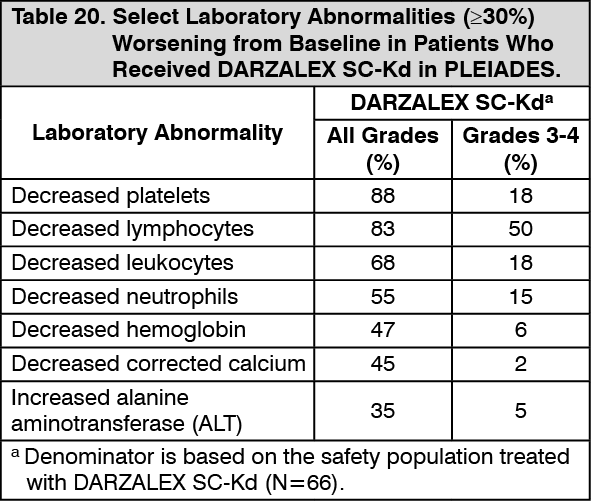 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image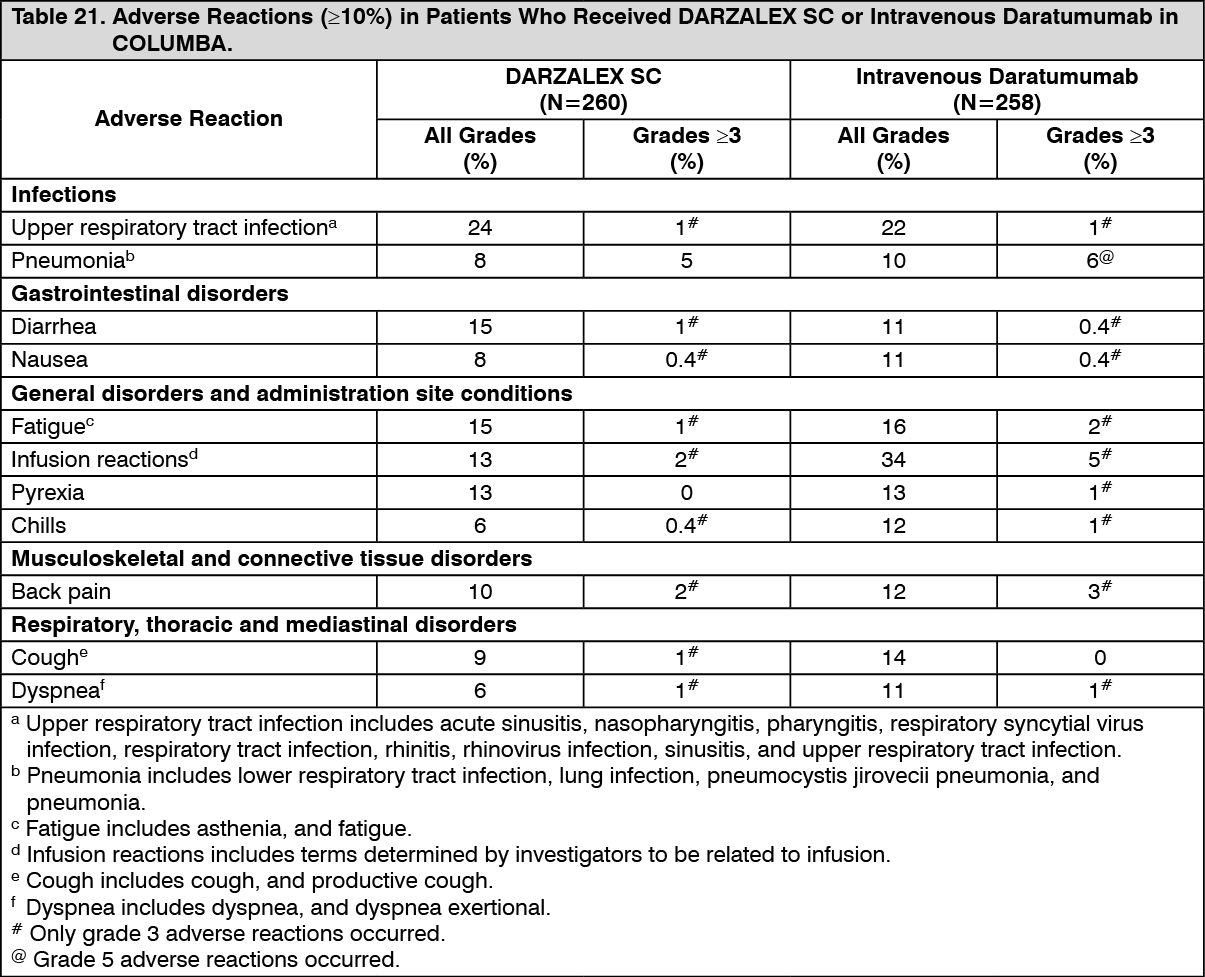 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image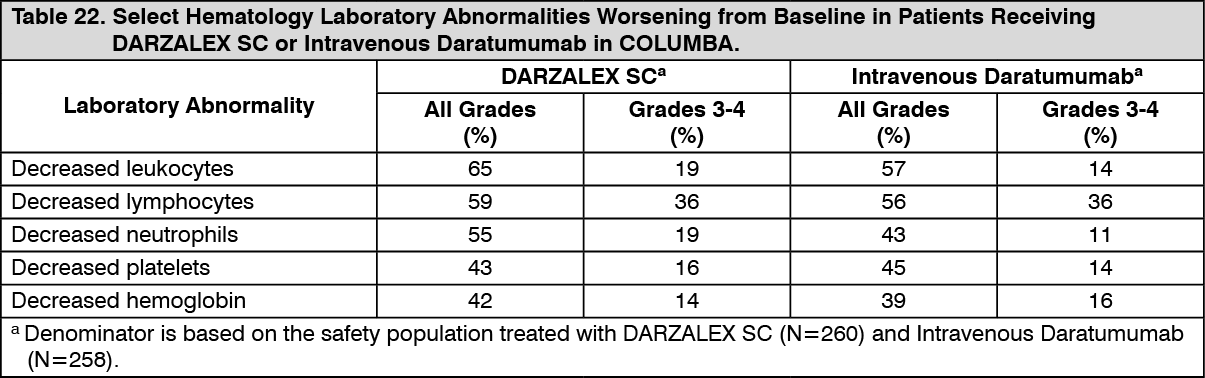 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image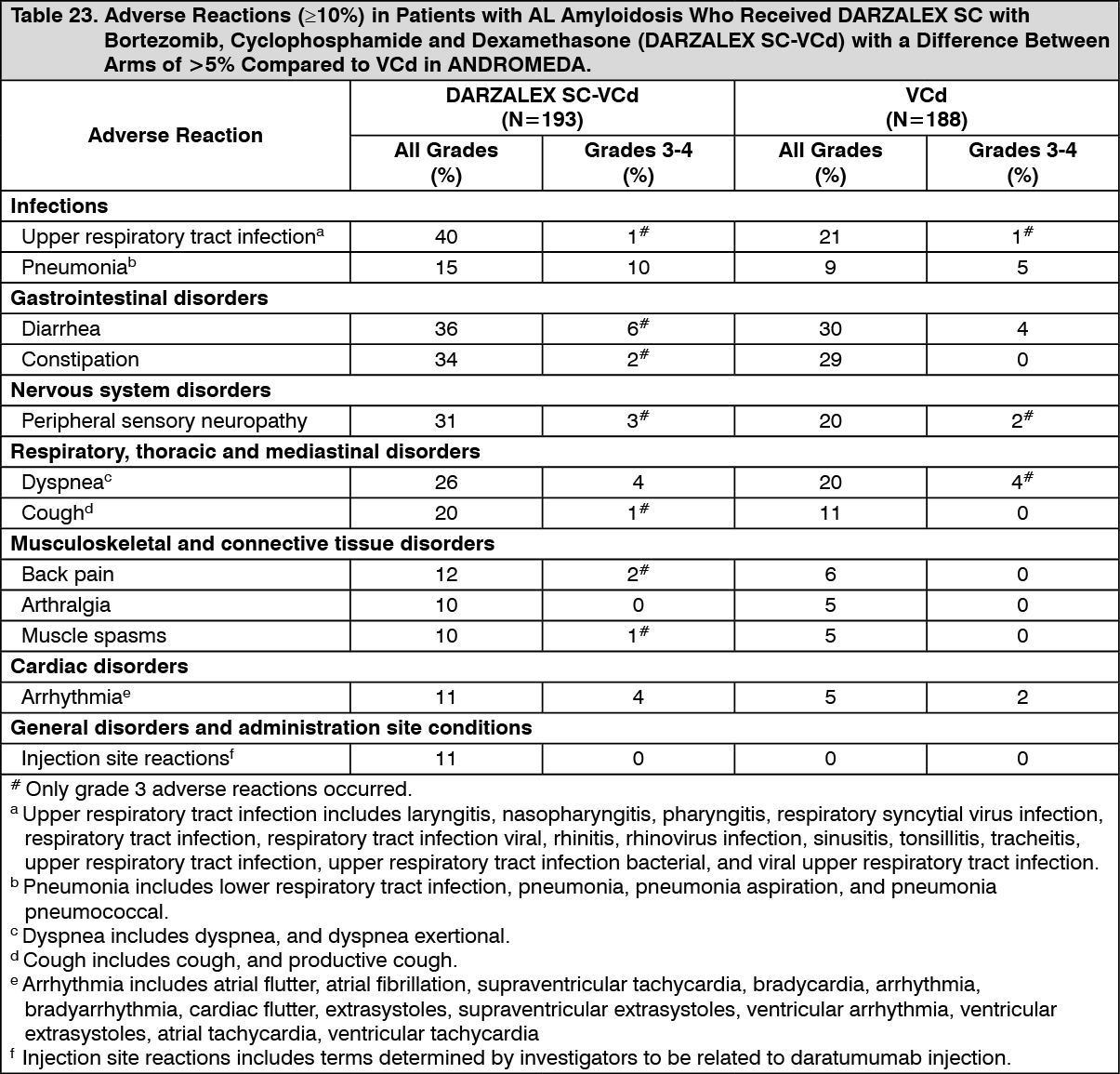 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image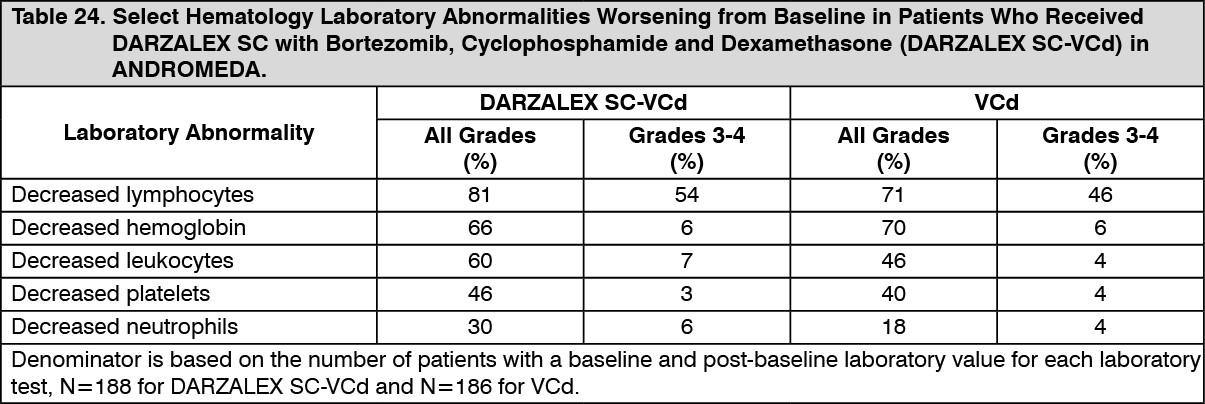 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out